Technology enabled care services are currently going through a significant period of change due to the digital switchover of telecommunications networks in the UK. This has major implications for alarm-based telecare, as existing analogue products and platforms are not optimised for use with these new fully digital (IP-based) networks. As legacy analogue telecare products are upgraded to digital equivalents and new data monitoring products become increasingly both the norm and the expectation, the well-established technologies used to allow devices to talk to each other are changing. This affects how devices communicate both within the home and with related monitoring services and telecare response services where they exist. This article discusses these changes and their impact on the sector, including how they will accelerate the adoption of new technology-enabled care and support service models and applications.
First and Second Generation TEC and the Digital Switchover
The digital switch-over process of the UK’s telecommunications infrastructure, initially announced in 2017 is now well underway and is due to be completed by December 2025. By then, the long-established analogue telephone service (the Public Switched Telephone Service or PSTN) will be decommissioned, as will ISDN services. These changes have significant implications for alarm-based telecare technology within the home, and for monitoring services more generally. Simultaneously, Fibre to the Premises (FTTP) is being rolled out across the country, linking homes to the core network using fibre-optic cable (‘full-fibre’ broadband), to replace copper wiring with a more resilient medium that enables data to flow at much faster speeds. To complicate matters further, the UK’s mobile network providers are in the process of retiring their 3G networks over the next year or two to focus on improvements in their 4G and 5G networks; these new networks also provide better, faster, and more reliable services with extremely low latency that enables real-time interactions to take place.
The telecare sector has responded to these challenges by investing in the development of digital alarm hubs which essentially replicate the key features of the analogue units they are replacing. They are designed primarily to manage the transition period as service users are switched over to new digital services. The shift to a digital network has significant implications for how voice-based telephone services are provided and for services such as telecare, that currently rely on the use of the legacy analogue phone network (PSTN); namely:
- The phone connection will fail in the event of a power-cut as an independent power supply is no longer available as it was with the PSTN. Digital voice-based services will be provided through a broadband hub, which is mains-powered. This has implications for both telecare alarm equipment connected using the hub and for the ability to contact the emergency services using the 999 service. In addition, properties with a FTTP ‘full fibre’ broadband connection, will also lose power to the Optical Network Terminal (ONT) that is required between the fibre optic cable to the home and the connection to the hub.
- Analogue alarm equipment, such as telecare alarm hubs, may not operate reliably over the new digital network because they use analogue alarm protocols based on DTMF ‘tone-based’ signalling. These tones are not always reliably transmitted over digital networks, resulting in alarm call failures due to handshaking errors between alarm hubs and the monitoring centre. This leads to a need for multiple call attempts, and a delay, before a successful alarm call is received at the monitoring centre.
- Most modern analogue alarm hubs (newer than about ten years old) should work over digital networks using the Analogue Terminal Adapter of the broadband router, but some older equipment will not work at all; and will need to be discarded and upgraded. It is expected that as the digitisation of the network is extended across the UK, the rate of analogue alarm call failures will increase.
- Existing wired phone extensions in the home will not work, although most people now use wireless DECT handsets to support multiple phones in their home (these will also fail in the event of a power-cut).
The impact of the changes described above for dispersed telecare are being addressed with the following approaches:
- The use of a battery backup solution to provide power in the event of a power cut for a brief period (usually about an hour). This would need to power the broadband router (if in use) and the optical network terminal used with a full-fibre connection. If a DECT base station is used for supporting legacy phone handsets throughout the home (connected via the Analogue Terminal Adaptor (ATA) of the broadband router), then this would also need to be powered to allow these to be used. Telecare alarm equipment will have its own internal backup battery (EU/UK social alarm standards currently require 24-hour continued operation in the event of local power failure) and should also have an alternative communications route either with a dual SIM approach, or by using a broadband landline connection. Of course, if a power-cut covers an extended area, it might also impact the local cabinet, exchange, and mobile masts. Whilst exchanges will have access to a backup power supply, mobile masts have mixed access, with variable up-times. Ofcom are in the process of reviewing their guidance on this issue with a view to improving the resilience of telecom networks.
- New digital telecare hubs are now available that support digital IP-based alarm protocols that are designed to work over IP-based networks. However, these can be twice as expensive as their analogue counterparts, offer little additional functionality (other than remote programming and device management) and are not always fully interoperable with all alarm monitoring platforms, even when the suppliers of the system claim to support a particular alarm protocol. Digital grouped living platforms are also available that support IP-based alarm protocols and networks. Furthermore, there are cloud-based services which function as a bridge between the analogue and digital/IP worlds. These work by receiving analogue alarm protocols and converting them to IP-based alarm protocols for onward transmission to the monitoring service of choice.
- DECT handsets are still supported by connecting the DECT base station to the Analogue Terminal Adapter (ATA) of the broadband router. There are also Digital Voice handsets that link to a DECT base station built into broadband routers that support digital voice services. Some providers also support the use of a digital voice app that can be used by several users, which also allows its use outside of the home.
There has recently been some negative press for both the telecom and telecare sectors concerning the switchover process because of example situations which have not been well managed. Consequently, Telecoms providers have signed a new Charter committing to “concrete measures to protect vulnerable households”, with the following key commitments:
- All providers have agreed to not forcibly move customers onto the new network unless they are fully confident, they will be protected.
- Providers will conduct additional checks on customers who have already been forcibly migrated to ensure they do not have telecare devices that the provider was not aware of, and if they do, to ensure suitable support is provided.
- No telecare users will be migrated to digital landline services without the provider, customer, and telecare company confirming they have a compatible and functioning telecare solution in place.
- Providers will be required to work to provide back-up solutions (battery systems) that go beyond regulator Ofcom’s minimum of one hour of continued, uninterrupted access to emergency services in the event of a power outage.
- They will collectively work with Ofcom and the UK government to agree a shared definition of ‘vulnerable people’ for this transition, so it is no longer dependent on the company and establishes an industry wide standard.
- Government will also continue to work with the telecare sector to reduce risk for users during the digital transition.
However, all alarm users do not automatically qualify as being vulnerable; users need to register as such with their communication provider. In response to situations where vulnerable people and other edge use cases where the transition to digital voice may not be straightforward by 2025, BT and Openreach are developing an additional phone line product called ‘SOTAP for Analogue’. This will not require a broadband connection and will also provide remote power (removing the need for battery backup). However, it is likely that the alarm transmission issues described above with analogue (DTMF) telecare hubs will remain.
ISDN services are also being decommissioned with implications for both grouped housing schemes and monitoring centres. Schemes typically use ISDN to provide shared connectivity for multiple dwellings with the monitoring centre. Likewise, many monitoring centres use ISDN to provide analogue alarm and voice telephony services. Monitoring centres will need to upgrade their analogue telephony with suitable digital broadband connectivity and support for IP-based digital voice services (using SIP) and associated IT support without further delay. They will also need to ensure that their alarm monitoring platform can handle the new digital alarm protocols and IP-based voice/telephony services. Many of the smaller centres have closed during the past few years as the cost of upgrading escalates.
3G+ TEC Applications
Third, fourth and fifth generation telecare services have moved the focus from alarms and voice-based interaction to continuous monitoring of activities and health parameters, with timely alerts replacing emergency alarms. Data-led applications depend on reliable wireless connectivity within the home, and then onward transmission using a wireless or landline broadband connection to cloud-based services and/or a monitoring service. Worn devices that support continuous operation will also make use of wireless connectivity to provide on-going support when out and about. Following data analysis or call handling, a tailored response will be provided by a blend of people-based support and digital applications, as appropriate. Figure 1 shows an overview of the key wireless technologies of relevance for use both within and outside the home.
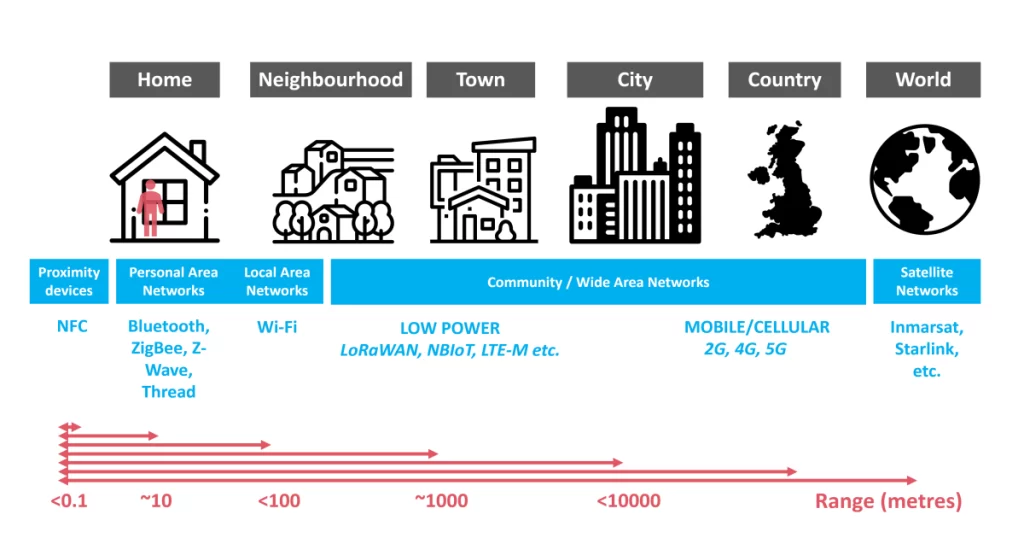
Within the home, individual devices typically connect wirelessly to a local hub. This provides connectivity out of the home using either an integrated 4G+ mobile data connection or a landline broadband connection, or both to provide redundant capacity if one channel should fail. The digital hub itself could be a smartphone or a tablet computer but is usually a bespoke product with varying degrees of interaction possible with the end-user. Peripherals can be connected to a hub using wired connections, including powerline network adapters, although by far the most common method is wireless radio. Whilst traditional telecare devices use licensed radio channels specifically for alarm use, new hub designs, such as the ones shown in Figure 2, are more likely to support newer consumer wireless technologies that have their roots in smart home and Internet of Things (IoT) applications.

They each have slightly different characteristics; a summary of some of the key technologies is provided below:
- NFC – Near Field Communication is used over very short distances, typically a few centimetres, to securely transfer small amounts of data. It is the technology used with contactless payments and can be used to log visits to a home by professional carers or to provide access to a property. Information is usually transferred in one direction only.
- Bluetooth/Bluetooth LE – Bluetooth is commonly used for streaming audio over a relatively short distance (it has a typical working range of about 10m, depending on local conditions). Bluetooth Low Energy (LE) is used for transmitting small packets of data between devices. Examples include transmitting data between a medical device or fitness tracker and a smartphone app or to control devices such as a smart light bulb.
- ZigBee/Z-Wave/Thread – these are low-power technologies that allow devices to communicate with each other using mesh networking to help extend coverage across the home. They are commonly used in smart home and IoT applications They are used to transmit data or commands between devices e.g., room temperature data from a sensor to the main thermostat controller; or an instruction to turn on the light in the hallway following a command received from a sensor or a voice instruction through a smart speaker such as an Amazon Echo device. Significantly, Thread, the newest technology, is based on the Internet Protocol (IP) so that it can connect directly to other IP-enabled devices throughout the home without a bridge device (reducing costs). It is the radio protocol that the new smart home connectivity standard – Matter – is based on. Matter has been conceived to standardise wireless connectivity in smart homes and is likely to become the leading technology, but as it is still relatively new it will take time for supported devices to become widely available.
- Wi-Fi – Wi-Fi is a ubiquitous wireless communication technology that allows devices to connect to the internet and communicate with each other wirelessly. It enables devices such as smartphones, tablets, laptops, smart TVs, and smart home devices to establish a wireless connection to a local area network (LAN) or the Internet. It provides high-speed data transmission and allows users to access online services, browse the web, stream media, and transfer files without the need for physical cables. It is relatively power-hungry and so is not generally suitable for battery-powered devices.
The key lesson is that new-generation (4G+) systems use commercially available ‘commodity’ products resulting in lower cost and more aesthetically pleasing devices. There are many suppliers of sensors and peripherals that use smart home wireless technology to communicate with a hub. So, there is no reliance on a single supplier, and it opens the possibility of in-home interoperability between products of different manufacturers. The widespread adoption of Matter as a smart home connectivity standard might go some way to achieve in-home interoperability between devices.
Low Power Wide Area Networks (LPWANs)
LPWANs are an interesting ‘third way’ of linking sensors to cloud-based services. Significantly, they do not require a hub in the home to link sensors to the cloud, rather sensors link directly to the cloud via a Low Power Wide Area Network (LPWAN). They are intended for applications with small messages only a few times per hour rather than data-heavy applications like streaming, and hence they are ideal for event-based and low data rate sensor-based applications. They make use of gateways that provide a wireless connection between devices and cloud-based services over the Internet. The operating range of a LPWAN gateway varies from a few kilometres in urban areas to over 10 km in rural settings. There are two groups of technologies – ones built around specific gateway infrastructure and those built on existing cellular (mobile) networks. Significantly, there is no need for a hub in the home for LPWAN enabled devices providing it is within range of an existing gateway/cell. There are again several competing technologies, examples include:
- LoRaWAN – this uses open-source technology and can transmit over unlicensed frequency bands. Designed for the Internet of Things (IoT), it works well indoors, is ultra-low power –supporting a battery life of up to 10 years – and is especially valuable for applications in remote areas where cellular networks have poor coverage. The gateways, with receiving antenna, can be situated on the roofs of municipal or community buildings that can provide both power and connectivity to the Internet.
- NBIoT/LTE-M – these are based on existing mobile phone technologies and networks, though availability around the country remains patchy. Narrow Band IoT (NBIoT) is a standards based LPWAN technology that supports very low data rates and is ideal for use with static sensors. It is low power and supports a battery life of up to 10 years. It has excellent indoor coverage and is scalable, supporting many device connections per cell. It also benefits from all the security and privacy features of mobile networks, such as support for user identity confidentiality, entity authentication and data integrity. LTE-M offers higher data rates, voice capabilities, SMS messaging, improved security and supports more simultaneous connections than NBIoT. Individual sensors require their own SIM card and data plan to connect to the network.
LoRaWAN has been around for longer than NBIoT, consequently it is more mature and has a greater choice of devices which are generally lower cost than NBIoT due to its wider adoption, although this may level out as NBIoT becomes more established. The range of LPWANs means that a single gateway or cell can monitor thousands of devices. Potentially, all properties in an entire county could be monitored through a relatively small number of gateways or cells. The result is that these solutions are readily scalable, offering opportunities to provide services to entire communities, thus enhancing the opportunities for the early detection of issues. Forward-looking local authorities and housing associations are already using these networks for monitoring homes both in urban areas and in rural environments.
Benefits of LPWAN for Smart Cities and Communities
Both activity and remote vital signs monitoring systems will increasingly employ lower-cost, generic sensors that meet relevant industry standards for connectivity, data-sharing, and security. They are usually provided only when they are required (preferably after a needs assessment). Installation is then organised, often leading to a delay in hospital discharge. Procedures for the maintenance, testing and withdrawal of the sensor devices will also have to be arranged.
For grouped housing that is managed by a social landlord, an alternative approach might involve the installation of devices in all properties so that all households can be monitored if necessary. Following appropriate assessment and consent, the relevant sensors could be enabled to allow monitoring to be switched on, remotely, only when needed (and switched off when no longer required). LoRaWAN systems can provide the most cost-effective approach, especially where mobile coverage is poor and when monitoring is in one direction only.
As an example of wide-scale adoption, in France, smart metering for energy and water use is available through three competing long range, low power systems – LoRaWAN, NBIoT and Wize. The former has become the market leader with over 3.5 million systems deployed. This includes 350,000 in the Lyon district alone where the municipality has control of the system and the data. This is in line with a common theme where customers may prefer to use a private rather than a public network where management is performed by a local organisation or delegated to a third party on a contract basis. This approach enables that control remains local beyond the contract period.
Mobile Communications
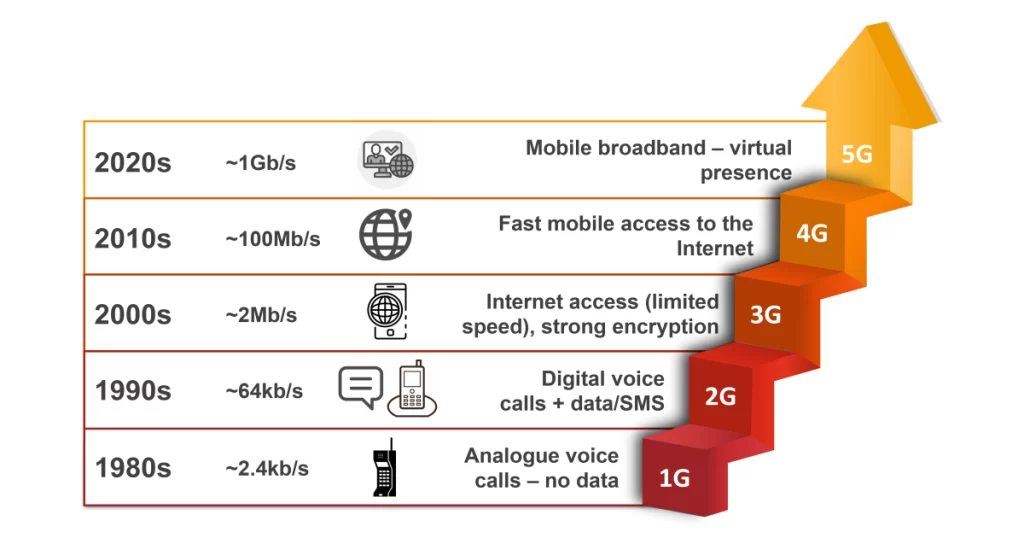
About once a decade, a new generation of mobile network technology is introduced that is faster and has less lag than the previous generation (see Figure 3). 4G mobile technologies and above enable more applications to be offered without the need for a fixed line broadband connection to the home, whilst also supporting the use of more data intensive applications when out and about. The earlier generations were used for basic telecare services but could not offer the speeds needed for two-way video calls, including the rapidly expanding market of remote patient monitoring.
In terms of speed, 4G and 5G mobile technologies are beginning to rival basic fixed-line broadband and, where available, can be provided quickly so that telecare services can be deployed as soon as a person is assessed as needing such support, e.g., following discharge from hospital. But there remain significant differences in the running costs – fixed line broadband is a much lower-cost option for on-going applications including the streaming of films and other video content. More generally, the situation may be complicated by the range of schemes available for fixed line broadband; homes where copper has been replaced by fibre offer the fastest speeds but at a higher cost. There are social tariffs available that enable people in receipt of certain eligible benefits such as income support, universal or pension credits to take advantage of Internet access using fixed-line or mobile connections.
The benefits of 5G will initially be seen in applications outside the home, especially in transport, where autonomous vehicles will be dependent on rapid communication for safe motoring. Ambulances and rapid response paramedics will be able to provide real-time ECG and other vital signs information for immediate and on-going analysis by doctors in the hospital.

More generally, the implications for social care and for community support will also be significant:
- Remote monitoring from the home using ‘tricorder’ devices that can be loaned to families could be useful in both paediatric and geriatric applications. Both Tytocare and Mediwand (see Figure 4) offer an integrated device that links to a physician, a paramedic or a hospital’s emergency department for triage or for follow-up assessment to avoid hospitalisation. Cameras within the devices enable real-time viewing of ear, nose and throat, for example.
- Physiotherapy/occupational therapy – a single professional may monitor multiple patients simultaneously for group exercises, increasing staff productivity and avoiding the need for travel by staff and patients. Similar sessions for social care applications are also enabled.
- Medication adherence – systems such as Paman, enable trained pharmacy staff to offer advice and monitor medication administration, thus improving outcomes.
- Automatic responses to emergencies can be initiated – smart home devices (see above) can make situations safe, while interface devices, such as Care Messenger can be used for triage.
- Control of robotic devices – future aids in the home will be capable of autonomously performing most domestic tasks but will need connectivity to cloud-based services to ensure that they can operate safely and deal successfully with changing circumstances.
In each of the above cases, communication needs to be fast and bi-directional using either a fixed-line broadband or 4G+ mobile connection to be successful.
Conclusions
The changes described in this article are technology-focussed but have significant consequences for how technology-enabled care services are currently implemented and how new applications can be delivered going forward. These are summarised below:
- The shift to fully digital (IP) telecommunications networks means that elements of analogue infrastructure, including older dispersed alarm units, may not work reliably. The adoption of digital hubs and monitoring platforms will solve alarm transmission issues but will also introduce new challenges.
- Both digital telephony and alarm services are reliant on a functioning internet connection. If this fails, then so does the ability to communicate with a monitoring or a response service. For landline connections, internet access can fail due to a local issue such as a power cut or some technical problem elsewhere across the network. The former can be successfully mitigated by using devices that can switch automatically to battery operation in the event of a local power failure. The latter requires an alternative communications path, such as a built-in mobile data connection.
- The uncertainty surrounding fixed-line broadband connections has led to the use of hubs that rely primarily on their own mobile data connection. They also have a battery backup capability, making them self-sufficient and easier to deploy – with no requirement for an existing landline connection. This is also true of 3G+ (non-alarm) data monitoring hubs.
- Some products circumvent the need for a local hub entirely by using sensors that can connect directly to low power wide area networks. This approach is sensible for providers of social housing and to local authorities who may wish to monitor both general needs housing and schemes designed primarily for older and more vulnerable tenants.
- The move to digital platforms has driven the development and adoption of industry standard digital alarm protocols which will help improve interoperability issues between home hubs and alarm monitoring centres. Whilst proprietary alarm protocols are still preferred by some manufacturers, the sector must move to commissioning systems that have been validated against the latest industry standards. This will ensure that products and systems from different manufacturers can work seamlessly together, thus reducing supplier tie-in. It will also enable replacement service providers to take over monitoring responsibilities more easily in the event of a business failure.
- This is not the case for 3G+ data monitoring products as there is currently no agreed coding standard for environmental and activity monitoring across the sector.
- In alarm-based telecare, the move to IP technology has not been extended to devices in the home, so interoperability between sensors and peripherals may still be some way off. However, in 3G+ data applications, the increasing use of off-the-shelf consumer IoT devices means that there is increased potential for interoperability to exist between devices.
- Emerging smart home standards like Matter will support improved interoperability between devices both at the radio and data description level, which will help open the in-home sensor/device market. This will lead to the ability to commission best-of-breed devices to work with any compatible hub.
- Home hubs are likely to become generic – providing basic access to the internet together with home networking and battery backup capabilities – with data analytics applied in the cloud. Product differentiation may include expanded user interface capabilities such as touchscreens or voice UI, supported with a bespoke or consumer-based intelligent agent.
- Future systems may use fixed line broadband or 5G wireless networks to provide the fast connection that will be necessary for virtual presence applications as well as HD video discussions, digital therapeutics and social/care robotics.
- In the meantime, commissioning bodies need to consider how the range of digital care and support applications that they use connect to the cloud and to other linked services.
The technological landscape of technology-enabled care, which has been stable for decades, is currently undergoing a seismic shift. This can be unsettling for service providers and commissioners who must manage the changeover process and its associated risks. It involves porting legacy systems over to the digital world but also keeping one eye to the future. Key to all of this is how these systems can be made to work together – preferably through an integrated platform – and thus enabling a truly data-driven service. Their ability to respond to alerts generated by the individual, their family and carers, or by smart equipment will also be critical to success.
These topics will form the basis of the next article in this series, on rethinking the role of monitoring in technology-enabled care.